Acknowledgement
The IORgait is a protocol from the Istituto Ortopedico Rizzoli and in particular, through the collaboration of Alberto Leardini and Maria Grazia Benedetti.
IORgait Purpose
IORgait is a gait analysis protocol and report that is expected to be a fundamental examination in current clinical practice. Various clinical gait analysis software is available commercially. IORgait is aimed at obtaining a compromise between the following contrasting criteria:
- Protocols for clinical gait analysis should pursue a thorough and reliable reconstruction of segment and joint kinematics based on subject-specific anatomical references on one hand, and rapid, simple, and practical procedures of data collection and reduction on the other hand, particularly when children are analysed.
- Anatomical reference frames should be defined using anatomical landmarks, and these should be chosen to be identified easily, preferably by external palpation, in a repeatable fashion.
- Report gait results using current international recommendations.
IORgait comprises three published protocols (described below):
- IORgait
- IORfoot
- IORtrunk
The IOR protocols have been validated clinically with links to the various publications in the next section.
|
|
- Leardini A, Sawacha Z, Paolini G, Ingrosso S, Nativo R, Benedetti MG.(2007)
- A new anatomically based protocol for gait analysis in children.
- Gait Posture. 2007 Oct;26(4):560-71
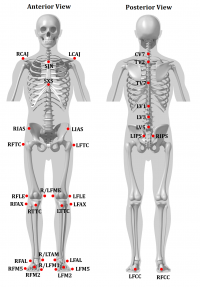
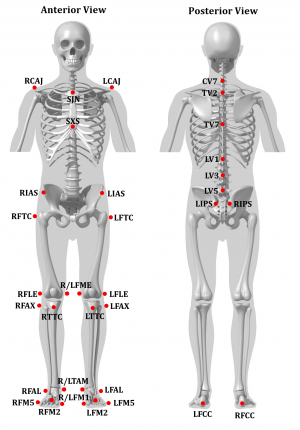
- Human movement analysis still suffers from the weakness of the currently used protocols for data collection and reduction. Reliable data comparisons and precise functional assessment require anatomically based definitions of the reference axes and frames, and therefore careful identification and tracking of the landmarks. When impaired children are analysed, the marker-set and other measurement procedures have to be minimised to reduce the time of the experiment and ensure patient collaboration. A new protocol is proposed for the analysis of pelvis and lower limb motion obtained as a compromise between these two requirements. A marker-set is proposed which involves the attachment of 22 skin markers, the calibration by a pointer of 6 anatomical landmarks, and the identification of the hip joint centre by a prediction approach. Anatomical reference frames and joint rotations are defined according to current recommendations. The protocol was assessed by analysing a single child in several repetitions by different examiners, and a population of 10 healthy children, mean age 9.7-years-old. The entire analysis was repeated after subtraction of the offset by static posture angles. The minimum and maximum means of the standard deviations from five examiners of the same child were respectively 2.1 degrees in pelvic obliquity and 6.8 degrees in knee rotation. The minimum and maximum means of the standard deviations from the 10 healthy children were 2.1 degrees in pelvic obliquity and 9.6 degrees in knee internal-external rotation. The protocol is feasible and allows 3D anatomical-based measurements of segment and joint motion and data sharing according to current standards.
|
|

|
- Leardini A, Benedetti MG, Berti L, Bettinelli D, Nativo R, Giannini S.(2007)
- "Rear-foot, mid-foot and fore-foot motion during the stance phase of gait."
- [Gait Posture. 2007 Mar;25(3):453-62.
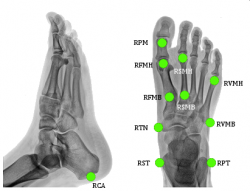
- This paper proposes a new protocol designed to track a large number of foot segments during the stance phase of gait with the smallest possible number of markers, with particular clinical focus on coronal plane alignment of the rear-foot, transverse and sagittal plane alignment of the metatarsal bones, and changes at the medial longitudinal arch. The shank, calcaneus, mid-foot and metatarsus were assumed to be 3D rigid bodies. The longitudinal axis of the first, second and fifth metatarsal bones and the proximal phalanx of the hallux were also tracked independently. Skin markers were mounted on bony prominences or joint lines, avoiding the course of main tendons. Trajectories of the 14 markers were collected by an eight-camera motion capture system at 100 Hz on a population of 10 young volunteers. Three-dimensional joint rotations and planar angles were calculated according to anatomically based reference frames. The marker set was well visible throughout the stance phase of gait, even in a camera configuration typical of gait analysis of the full body. The time-histories of the joint rotations and planar angles were well repeatable among subjects and consistent with clinical and biomechanical knowledge. Several dynamic measurements were originally taken, such as elevation/drop of the medial longitudinal arch and of three metatarsal bones, rear-foot to fore-foot rotation and transverse plane deformation of the metatarsus. The information obtained from this protocol, consistent with previous clinical knowledge, enhanced our understanding of the dynamics of the human foot during stance.
|
For more information about other multi-segment feet, here are summaries of other Multi-Segment Foot Models and
Kinetic Segment Foot Models.
|
|
- Leardini A, Biagi F, Merlo A, Belvedere C, Benedetti MG. (2011)
- "Multi-segment trunk kinematics during locomotion and elementary exercises."
- Clin Biomech (Bristol, Avon). 2011 Jul;26(6):562-71
- BACKGROUND: Motion of human trunk segments in healthy subjects during activities of daily living has been described either with oversimplified models or with cumbersome techniques of isolated anatomical complex. This study describes multi-segmental trunk motion based on a new technique which is a compromise between technical limitations, implied with the experiments, and clinical relevance.
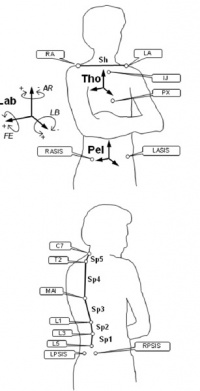
- METHODS: The thorax segment was tracked by the optimal spatial matching of four thoracic markers. The separate bi-dimensional shoulder line rotations and translations with respect to the thorax were calculated by markers on the two acromions. Spine motion was characterised by a 5-link-segment model from additional four skin markers, in the anatomical reference frame based on four pelvic spine markers. These 14 markers were tracked in 10 healthy subjects and one clinical case during static upright posture, chair rising-sitting, step up-and-down and level walking, and also during elementary flexion and extension, lateral bending, and axial rotation movements of the entire trunk.
- FINDINGS: Intra-subject repeatability over ten repetitions was found to be high for most of the measurements, with average standard deviations of less than 1.8° for all planar rotations at the spine, and less smaller than 1mm for shoulder translations. Large motion, albeit with different patterns, was found in all subjects, also revealing interesting couplings over the three anatomical planes.
- INTERPRETATION: Considerable subject-specific motion occurs at each of these different trunk segments in all three anatomical planes, in simple exercises and in motor tasks of daily living. Measurements taken with the present new trunk model in pathological subjects shall reveal corresponding patterns and ranges of motion in abnormal conditions.
|
Step by step instructions describing how to create these models be found on the Visual3D wiki.
|
A tutorial describing the IORgait model explicitly as a Visual3D model can be found here
|
|
|
A tutorial describing the IORgait model explicitly as a Visual3D model can be found here
|
|
Repeatability
|
Seo SG, Lee1 DY, Moon HJ, Kim SJ, Kim J, Lee KM, Chung CY and Choi1 IH (2014)
"Repeatability of a multi-segment foot model with a 15-marker set in healthy adults."
Journal of Foot and Ankle Research 2014, 7:24
- Background: Several 3D multi-segment foot models (MFMs) have been introduced for the in vivo analysis of dynamic foot kinematics. However, reproducibility of a model should be checked and ascertained before clinical utilization of a MFM. The purpose of this study was to determine the reliability of recently introduced MFM with a 15-marker set by assessing the participant’s stride-to-stride (intra-session) and visit-to-revisit (inter-session) repeatability.
- Methods: Twenty healthy adults with a mean age of 28.9 years (10 males and 10 females) were tested. Three representative strides from five separate trials were used for analysis from each session. Kinematic data of foot segmental motion was collected and tracked using the Foot3D Multi-Segment Software (Motion Analysis Co., Santa Rosa. CA). A retest was performed in the same manner at an interval of 4 weeks. Coefficients of multiple correlation (CMC) and intra-class correlation coefficient (ICC) were calculated in order to assess the intra-session and inter-session repeatability.
- Results: Inter-segment foot angles from healthy adults from a MFM with 15-marker set showed a narrow range of variability during the gait cycle. The mean intra-session ICC was 0.981 (±0.010), which was interpreted as excellent. The mean intra-session CMC was 0.948 (±0.027), which was interpreted as very good repeatability. The mean inter-session ICC was 0.886 (±0.047) and the mean inter-session CMC was 0.801 (±0.077), which were interpreted as excellent and good repeatability, respectively.
- Conclusion: We demonstrated a MFM with a 15-marker set had high intra-session and inter-session repeatability, especially in sagittal plane motion. We thought this MFM would be applicable to evaluation of the segmental foot motion during gait.
|
| Arnold JB, Mackintosh S, Jones S, Thewlis D. (2013)
"Repeatability of stance phase kinematics from a multi-segment foot model in people aged 50 years and older." |
| [Gait Posture. 2013 Jun;38(2):349-51.. |
- Confidence in 3D multi-segment foot models has been limited by a lack of repeatability data, particularly in older populations that may display unique functional foot characteristics. This study aimed to determine the intra and inter-observer repeatability of stance phase kinematic data from a multi-segment foot model described by Leardini et al. [2] in people aged 50 years or older. Twenty healthy adults participated (mean age 65.4 years SD 8.4). A repeated measures study design was used with data collected from four testing sessions on two days from two observers. Intra (within-day and between-day) and inter-observer coefficient of multiple correlations revealed moderate to excellent similarity of stance phase joint range of motion (0.621-0.975). Relative to the joint range of motion (ROM), mean differences (MD) between sessions were highest for the within-day comparison for all planar ROM at the metatarsus-midfoot articulation (sagittal plane ROM 5.2° vs. 3.9°, MD 3.1°; coronal plane ROM 3.9 vs. 3.1°, MD 2.3°; transverse plane ROM 6.8° vs. 5.16°, MD 3.5°). Consequently, data from the metatarsus-midfoot articulation in the Istituto Ortopedico Rizzoli (IOR) foot model in adults aged over 50 years needs to be considered with respect to the findings of this study.
|
| Deschamps K, Staes F, Bruyninckx H, Busschots E, Jaspers E, Atre A, Desloovere K.(2012)
"Repeatability in the assessment of multi-segment foot kinematics." |
| [Gait Posture. 2012 Feb;35(2):255-60. |
- A recently published systematic review on 3D multi-segment foot models has illustrated the lack of repeatability studies providing evidence for appropriate clinical decision making. The aim of the current study was to assess the repeatability of the recently published model developed by Leardini et al. [10]. Foot kinematics of six healthy adults were analyzed through a repeated-measures design including two therapists with different levels of experience and four test sessions. For the majority of the parameters moderate or good repeatability was observed for the within-day and between-day sessions. A trend towards consistently higher within- and between-day variability was observed for the junior compared to the senior clinician. The mean inter-session variability of the relative 3D rotations ranged between 0.9-4.2° and 1.6-5.0° for respectively the senior and junior clinician whereas for the absolute angles this variability increased to respectively 2.0-6.2° and 2.6-7.8°. Mean inter-therapist standard deviations ranged between 2.2° and 6.5° for the relative 3D rotations and between 2.8° and 7.6° for the absolute 3D rotations. The ratio of inter-therapist to inter-trial errors ranged between 1.8 and 5.5 for the relative 3D rotations and between 2.4 and 9.7 for the absolute 3D rotations. Absolute angle representation of the planar angles was found to be more difficult. Observations from the current study indicate that an adequate normative database can be installed in gait laboratories, however, it should be stressed that experience of therapists is important and gait laboratories should therefore be encouraged to put effort in training their clinicians.
|
|
Caravaggi P, Benedetti MG, Berti L, Leardini A. (2011)
"Repeatability of a multi-segment foot protocol in adult subjects."
Gait Posture. 2011 Jan;33(1):133-5
- Despite the numerous protocols for multi-segment kinematic analysis of the foot, the literature is scarce regarding relevant measures of reliability. The aim of the present work was to assess the inter-trial, inter-session and inter-examiner variability of one of these protocols by an established method. The kinematics of the joints of the foot of two volunteers were analyzed by four examiners with different degrees of experience in three sessions, two-to-four weeks apart. In each session the data of five trials of level walking were collected and the rotations in the three anatomical planes between foot segments were calculated. The mean value over stance phase duration of the standard deviation of these rotations was calculated for groups of trials according to the statistical method as in Schwartz et al. [6]. For each rotation, the inter-examiner variability was larger than the inter-session, and the latter larger than the inter-trial. The inter-session variability was found in the same order of magnitude for standard lower limb protocols for the two expert examiners, but much higher for the inexperienced examiners.
|



